


There’s a familiar script that plays out every winter. You feel something in the back of your throat, or a slight heaviness behind your eyes, or you’re a bit more tired than the day warrants. You register it, briefly, then push through — get on with the evening, go to bed hoping you’ll wake up fine. Sometimes you do. Often enough, you wake up properly sick, and by then the assumption is that you’re in for it: rest, fluids, maybe some paracetamol, wait it out. The cold has arrived, and there’s not much to do but ride it through.
That assumption is understandable, and for most people it’s never really been questioned. The idea is that once a virus takes hold, the illness runs a more or less predetermined course. You can soften the symptoms, but the trajectory is set. Vitamin C might take the edge off. Echinacea might shave half a day off the end. But fundamentally, the virus is doing what viruses do, and you wait.
That picture isn’t wrong, but it’s incomplete. Both Chinese medicine theory and a growing body of Western research point to something most people overlook: the hours after you notice those early signs aren’t a waiting room. They’re a window — and what happens in that window can genuinely change what the next week looks like.
How Chinese medicine thinks about early illness

In Chinese medicine, getting sick isn’t a binary event. You’re not fine one moment and ill the next — it’s more like a negotiation between the body and whatever it’s been exposed to.
When a pathogenic factor first makes contact, it meets the body’s outermost layer of defence, what Chinese medicine calls the wei qi. This layer operates at the surface: the skin, the nasal passages, the upper respiratory tract. At this early stage the pathogen hasn’t penetrated deeply — it’s still at the boundary, and the body is actively trying to push it out. The symptoms you feel reflect that effort: slight chills, a stiff neck, a tickle in the throat, a runny nose that starts thin and clear. These aren’t signs that you’re sick. They’re signs that your body is mounting a response at the surface, and that the outcome is still being decided.
If the pathogen is expelled at this point, the illness never fully develops — you might feel slightly off for a day, then recover completely. But if it isn’t addressed and it lodges deeper, things change. The cough drops into the chest, body aches intensify, fever climbs, fatigue sets in properly. At this stage the pathogen has moved past the surface defences, and the treatment required to shift it is more complex and takes longer.
This is why practitioners have always placed such emphasis on speed. The clinical tools available at the early stage are relatively straightforward — specific herbal formulas that support the body’s own expulsive effort, chosen according to whether the presentation looks more cold or more hot. The task is to reinforce what the body is already doing, while the job is still manageable. Once the illness has moved inward, the clinical picture becomes layered, and treatment needs to address several things at once. It’s less about killing the bug and more about helping the body close the door before the bug settles in.
Western research has been arriving at a similar conclusion
One of the more useful things to come out of the COVID era is a much sharper picture of what happens in the first hours and days of a respiratory viral infection. The details are described in different language, but the practical conclusion lines up remarkably well.
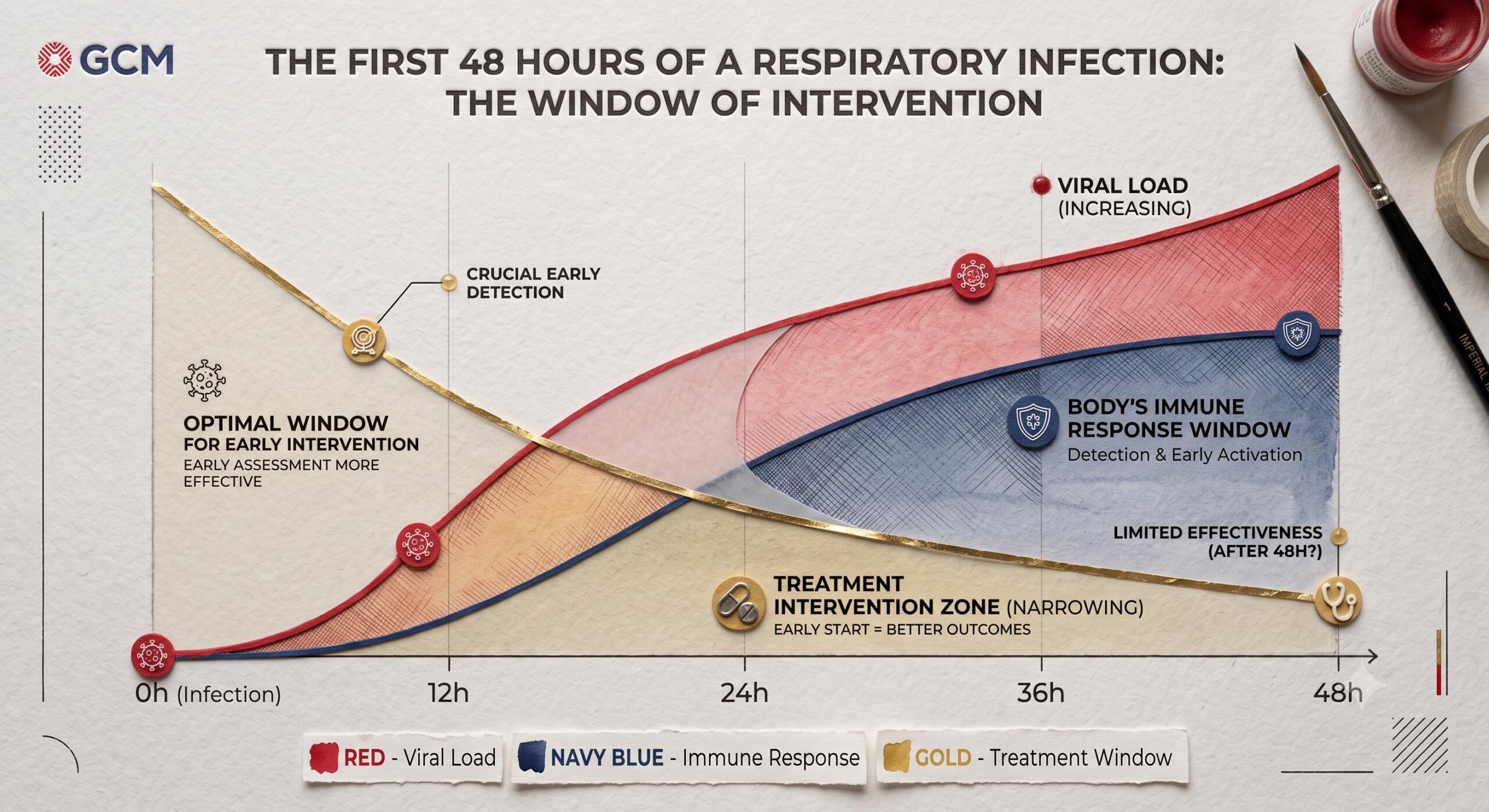
We now know that viral load in respiratory infections tends to peak early. Research on SARS-CoV-2 published in PNAS showed viral load typically peaking within the first few days of symptoms, sometimes even before symptoms appeared (Néant et al., 2021). The body’s encounter with the virus is at its most intense right at the start — not a slow build, but a front-loaded, critical period.
This is exactly why antivirals like oseltamivir (Tamiflu) and nirmatrelvir–ritonavir (Paxlovid) only work when taken early. Oseltamivir reduces symptom duration by one to two days when started within 48 hours of onset, and is most effective within the first six to twelve. In hospitalised influenza patients, early treatment cut the risk of death roughly in half compared with late treatment (Surie et al., 2024). Paxlovid’s benefit for COVID-19 follows the same time-dependent pattern (Lewnard et al., 2024). These drugs don’t work because they’re powerful enough to override an established infection — they work because they intervene while the body’s encounter with the virus is still in its early, decisive phase. Once that window closes, even pharmaceutical antivirals lose most of their effect.
The body’s own front-line defence follows the same logic. A striking 2023 study found that the nasal mucosa responds to viral contact by releasing extracellular vesicles that act as decoys, drawing the virus away from actual cells (Huang et al., 2023). This response is rapid and effective — but the same study found it was significantly impaired by cold air. When nasal tissue was exposed to a temperature drop of around 5°C, the vesicle response fell by nearly 42%. For anyone who’s wondered whether there’s a real biological reason people get more respiratory infections in winter, beyond simply spending more time indoors, this is a strong candidate: cold air appears to compromise one of the nose’s primary antiviral mechanisms.
Meanwhile, the innate immune system’s interferon response in the first 24 to 48 hours is critical. When it’s strong and well-timed, viral replication is contained; when it’s delayed or insufficient, the virus gains a foothold and replication outpaces the immune response (Li & Wang, 2022). The pattern holds: the body’s best chance of containing a respiratory virus is concentrated in the opening hours.
Even herbal early intervention has been tested in this framework. A quadruple-blinded randomised controlled trial on Andrographis paniculata for upper respiratory tract infections found that early intervention reduced sick leave by over 21% and measurably eased symptoms from the second day of treatment (Hu et al., 2021). What makes this study notable is that it specifically tested early versus late intervention, and found timing was a significant factor in the outcome.
Different explanations, same practical point
Chinese medicine describes the early phase of a respiratory illness as a pathogen at the body’s surface, still within reach of its outermost defences and relatively easy to expel. Western immunology describes a window in which mucosal immunity, interferon signalling, and viral load dynamics are all in flux and still responsive to intervention. The language differs, and the proposed mechanisms differ. But the practical conclusion is the same: the first hours and days are when intervention has the most leverage.
For patients, the value isn’t in choosing one framework over the other — it’s in recognising the pattern both are pointing to. That feeling of something coming on is not trivial, and it’s not hypochondria. It’s the body flagging that a negotiation is underway, and acting in those early hours is not wishful thinking.
Chinese medicine has a long clinical tradition of distinguishing early-stage from established illness, and the herbal strategies used at each stage differ considerably. A practitioner’s job in those first hours is to identify what kind of pathogen is involved, whether the presentation is running cold or hot, and to support the body’s response in a targeted way while the task is still relatively contained.
What this means for you

The practical takeaway is simple: pay attention to the early signals — the scratchy throat, the slight chill across the back of the neck, the fatigue that feels different from ordinary tiredness. These are worth responding to, not pushing through.
Give your body its best chance of mounting an early defence: rest, warmth, fluids, and lightening your load for the day. If you have access to a Chinese medicine practitioner, seeing them at this stage — rather than waiting until you’re three days into a full-blown cold — gives them the best chance of helping. The herbal strategies used early on are quite different from what’s appropriate once illness has progressed, which is why practitioner guidance matters. You could even ask your practitioner for a herbal kit to keep at home or take when you travel, with instructions on when and how to use it. Having something on hand for those first few hours turns acting early from a good intention into a realistic option.
This isn’t about replacing what already works. Rest, fluids, keeping warm, and seeing your GP when appropriate are all still good sense. Chinese medicine offers an additional framework for acting in that early window, when most people default to waiting.
If you’re in Geelong and you feel something coming on, give us a call. We’d rather see you on day one than day five.
Book an initial consultation through red button above, or call (03) 5221 8822.
References
Hu, X.Y. et al. (2021). Early intervention with Kan Jang to treat upper-respiratory tract infections. Journal of Traditional and Complementary Medicine, 11(6), 552–562.
Huang, D. et al. (2023). Cold exposure impairs extracellular vesicle swarm-mediated nasal antiviral immunity. Journal of Allergy and Clinical Immunology, 151(2).
Lewnard, J.A. et al. (2024). Public health impact of Paxlovid as treatment for COVID-19, United States. Emerging Infectious Diseases, 30(2).
Li, D. & Wang, M. (2022). Innate immune response in respiratory system. Viruses.
Néant, N. et al. (2021). Modeling SARS-CoV-2 viral kinetics and association with mortality in hospitalized patients. PNAS, 118(8).
Surie, D. et al. (2024). Benefit of early oseltamivir therapy for adults hospitalized with influenza A. Clinical Infectious Diseases, 81(1).
